Objective: Age, Risk factors, and Troponin (HEART), Thrombolysis in Myocardial Infarction (TIMI), and Score, and Global Registry of Acute Coronary (GRACE) Scores are critical for identifying patients at risk for major adverse cardiac events (MACE), guiding timely interventions, and optimizing resource utilization. This study aimed to evaluate the comparative utility of these three scoring systems in predicting MACE in patients visiting the emergency department (ED).
Material and Methods: This prospective observational study included 502 adult patients visiting the ED with chest pain of a tertiary hospital between December 2014 and March 2015. HEART Score, TIMI, GRACE Score were evaluated for MACE over a 14-day and six-week, period. Data collected included demographic characteristics, clinical findings, laboratory results, and outcomes such as myocardial infarction, coronary angiography, revascularization, and mortality. Statistical significance was set at p<0.05.
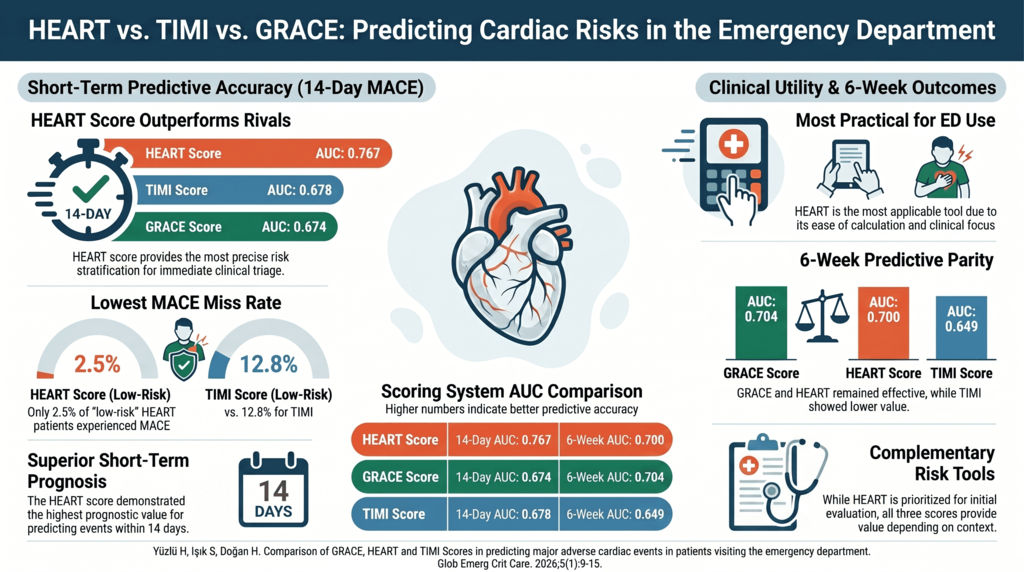
Results: At 14-day follow-up, the HEART Score identified 192 patients as “low risk”, of which 2.5% missed MACE. The GRACE Score identified 276 patients as “low risk”, of which 10.5% missed MACE. The TIMI Score identified 288 patients as “low risk”, of which 12.8% missed MACE. The area under the curve (AUC) for HEART Score, TIMI Score, and GRACE Score for 14-day MACE was calculated as 0.767, 0.678, and 0.674. In addition, the AUC for HEART Score, TIMI Score, and GRACE Score for MACE at 6-week follow-up was calculated as 0.700, 0.649 and 0.704.
Conclusion: The HEART Score demonstrates higher prognostic value for predicting MACE within 14 days than the TIMI and GRACE Scores in patients visiting the ED with chest pain. The TIMI Score has lower prognostic value for predicting MACE over a 6-week period compared to the HEART and GRACE Scores.
Keywords: TIMI Score, GRACE Score, HEART Score, chest pain, emergency department

 , Seyhmus Işık1
, Seyhmus Işık1